















Drug-Eluting or Bare-Metal Stents for Coronary Artery Disease
List of authors.
Committees, study centers, and investigators participating in the Norwegian Coronary Stent Trial (NORSTENT) are listed in the Supplementary Appendix, available at NEJM.org.
Abstract
Background
Limited data are available on the long-term effects of contemporary drug-eluting stents versus contemporary bare-metal stents on rates of death, myocardial infarction, repeat revascularization, and stent thrombosis and on quality of life.
Methods
We randomly assigned 9013 patients who had stable or unstable coronary artery disease to undergo percutaneous coronary intervention (PCI) with the implantation of either contemporary drug-eluting stents or bare-metal stents. In the group receiving drug-eluting stents, 96% of the patients received either everolimus- or zotarolimus-eluting stents. The primary outcome was a composite of death from any cause and nonfatal spontaneous myocardial infarction after a median of 5 years of follow-up. Secondary outcomes included repeat revascularization, stent thrombosis, and quality of life.
Results
At 6 years, the rates of the primary outcome were 16.6% in the group receiving drug-eluting stents and 17.1% in the group receiving bare-metal stents (hazard ratio, 0.98; 95% confidence interval [CI], 0.88 to 1.09; P=0.66). There were no significant between-group differences in the components of the primary outcome. The 6-year rates of any repeat revascularization were 16.5% in the group receiving drug-eluting stents and 19.8% in the group receiving bare-metal stents (hazard ratio, 0.76; 95% CI, 0.69 to 0.85; P<0.001); the rates of definite stent thrombosis were 0.8% and 1.2%, respectively (P=0.0498). Quality-of-life measures did not differ significantly between the two groups.
Conclusions
In patients undergoing PCI, there were no significant differences between those receiving drug-eluting stents and those receiving bare-metal stents in the composite outcome of death from any cause and nonfatal spontaneous myocardial infarction. Rates of repeat revascularization were lower in the group receiving drug-eluting stents. (Funded by the Norwegian Research Council and others; NORSTENT ClinicalTrials.gov number, NCT00811772. opens in new tab.)
Results
Patients and Follow-up
Figure 1.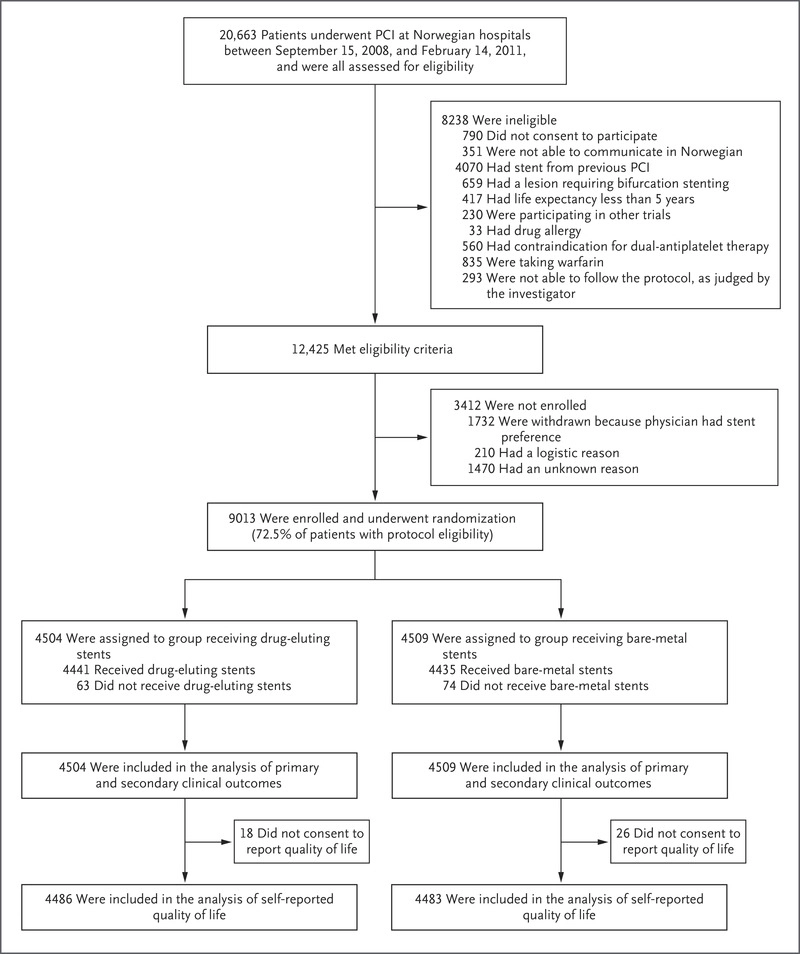 Figure 1. Enrollment, Randomization, and Follow-up.
Figure 1. Enrollment, Randomization, and Follow-up.All the patients who were treated with percutaneous coronary intervention (PCI) at Norwegian hospitals from September 15, 2008, through February 14, 2011, were considered for enrollment in the Norwegian Coronary Stent Trial (NORSTENT). Of the 12,425 patients with protocol eligibility, 9013 (72.5%) underwent randomization, with 4504 assigned to receive drug-eluting stents and 4509 assigned to receive bare-metal stents. All the patients were included in the intention-to-treat analyses of the clinical outcomes, and a total of 8969 patients were included in the analyses of disease-specific quality of life.
Table 1.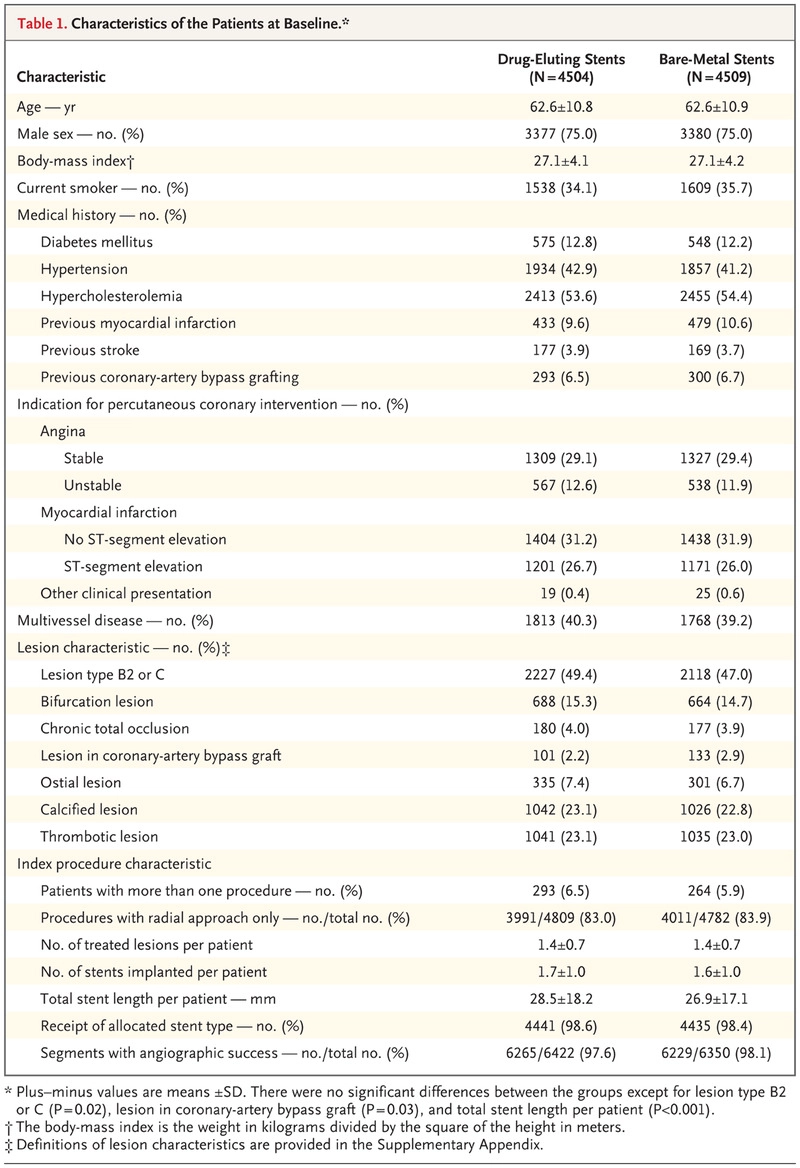 Table 1. Characteristics of the Patients at Baseline.
Table 1. Characteristics of the Patients at Baseline.From September 15, 2008, to February 14, 2011, a total of 20,663 patients underwent PCI in Norway. Of the 12,425 patients who were eligible to participate in the trial, 9013 (72.5%) underwent randomization (Figure 1). The two study groups were well balanced for most clinical characteristics (Table 1), although there were imbalances in total stent length, lesion type (see the Supplementary Appendix), and the proportion of lesions in coronary-artery bypass grafts. In the group receiving drug-eluting stents, 82.9% of the patients received everolimus-eluting stents and 13.1% received zotarolimus-eluting stents. All the patients in the group receiving bare-metal stents underwent placement of contemporary devices with thin struts. The names and manufacturers of all types of stents that were placed at baseline are provided in Table S1 in the Supplementary Appendix.
The median follow-up time was 59 months (range, 1 day to 76 months). No patients were lost to follow-up with respect to death, but the completeness of clinical follow-up was uncertain for 5 patients. The response rate to the quality-of-life questionnaire was 91% at 6 months, 88% at 1 year, 84% at 2 years, 82% at 3 years, 80% at 4 years, and 78% at 5 years.
Study Outcomes
Table 2.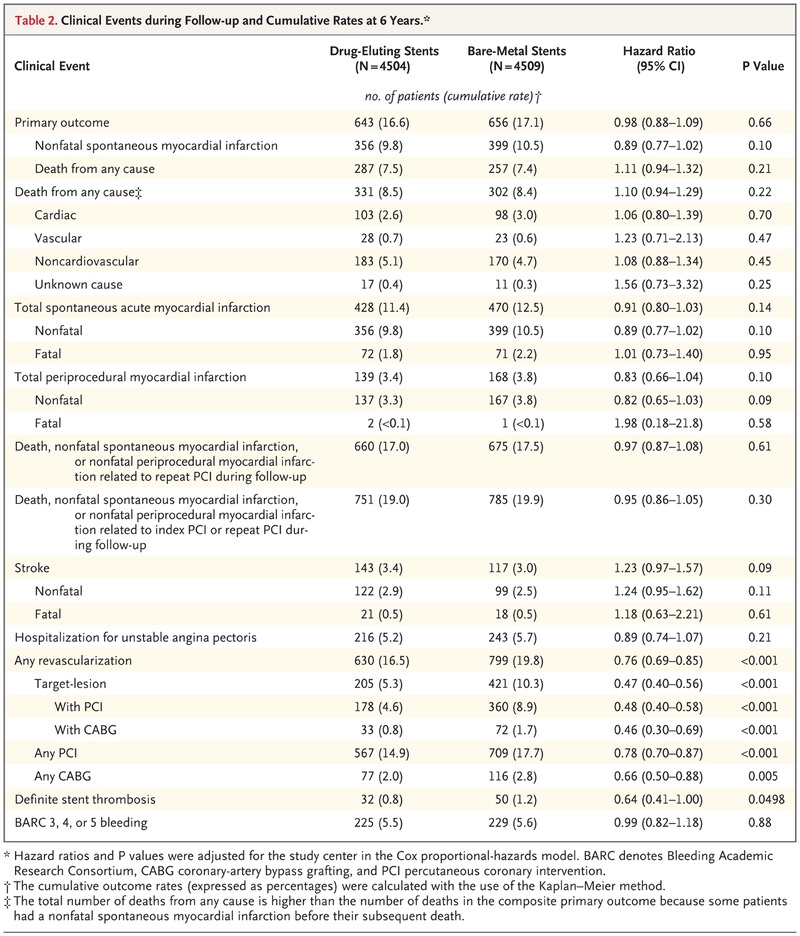 Table 2. Clinical Events during Follow-up and Cumulative Rates at 6 Years.Figure 2.
Table 2. Clinical Events during Follow-up and Cumulative Rates at 6 Years.Figure 2. 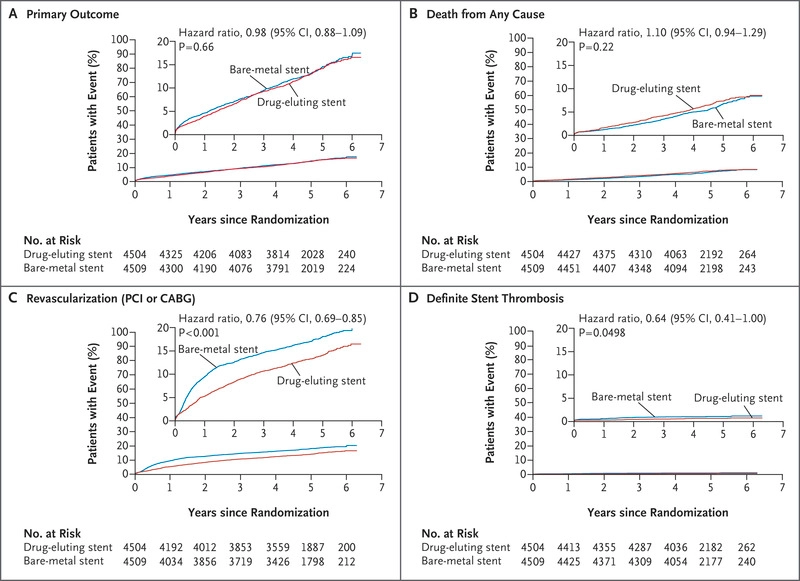 Figure 2. Clinical Outcomes.
Figure 2. Clinical Outcomes.Shown are Kaplan–Meier curves for patients receiving drug-eluting stents and those receiving bare-metal stents for the primary composite outcome of death from any cause and nonfatal spontaneous myocardial infarction (Panel A), death from any cause (Panel B), any revascularization with percutaneous coronary revascularization (PCI) or coronary-artery bypass grafting (CABG) (Panel C), and definite stent thrombosis, as assessed according to the criteria of the Academic Research Consortium (Panel D). The insets show the same data on an expanded y axis.
At 6 years, the rate of the primary composite outcome of death from any cause and nonfatal spontaneous myocardial infarction was 16.6% in the group receiving drug-eluting stents and 17.1% in the group receiving bare-metal stents (hazard ratio, 0.98; 95% CI, 0.88 to 1.09, P=0.66) (Table 2 and Figure 2). There was also no significant between-group difference in the primary outcome after adjustment for baseline imbalances in smoking status, hypertension, history of myocardial infarction, target-lesion type, and total stent length (data not shown). The results for the primary outcome were consistent in subgroups defined according to demographic, clinical, lesion, and procedural characteristics (Fig. S1 in the Supplementary Appendix).
There were no significant between-group differences in the rates of the individual components of the primary outcome. There were no significant differences between the study groups in the rates of death from cardiac, vascular, or noncardiovascular causes, in the rates of stroke (Fig. S2 in the Supplementary Appendix), or in the rates of hospitalization for unstable angina.
At 6 years, the cumulative rate of spontaneous myocardial infarction was 11.4% in the group receiving drug-eluting stents and 12.5% in the group receiving bare-metal stents (hazard ratio, 0.91; 95% CI, 0.80 to 1.03; P=0.14) (Table 2, and Fig. S2 in the Supplementary Appendix). The corresponding event rates for periprocedural myocardial infarction were 3.4% and 3.8%, respectively (hazard ratio, 0.83; 95% CI, 0.66 to 1.04; P=0.10). There were no significant differences between groups in the composite outcomes that included the primary outcome plus periprocedural myocardial infarction. The 28-day case fatality rate was 16% after spontaneous myocardial infarction, as compared with 1% after periprocedural myocardial infarction.
The 6-year rate of any revascularization was 16.5% in the group receiving drug-eluting stents and 19.8% in the group receiving bare-metal stents, an absolute risk reduction of 3.3 percentage points (hazard ratio, 0.76; 95% CI, 0.69 to 0.85; P<0.001) (Table 2 and Figure 2). On the basis of this result, 30 patients would need to be treated with drug-eluting stents rather than bare-metal stents to prevent one repeat revascularization. The difference in any revascularization between groups was driven by lower rates of target-lesion revascularization in the group receiving drug-eluting stents.
Figure 3.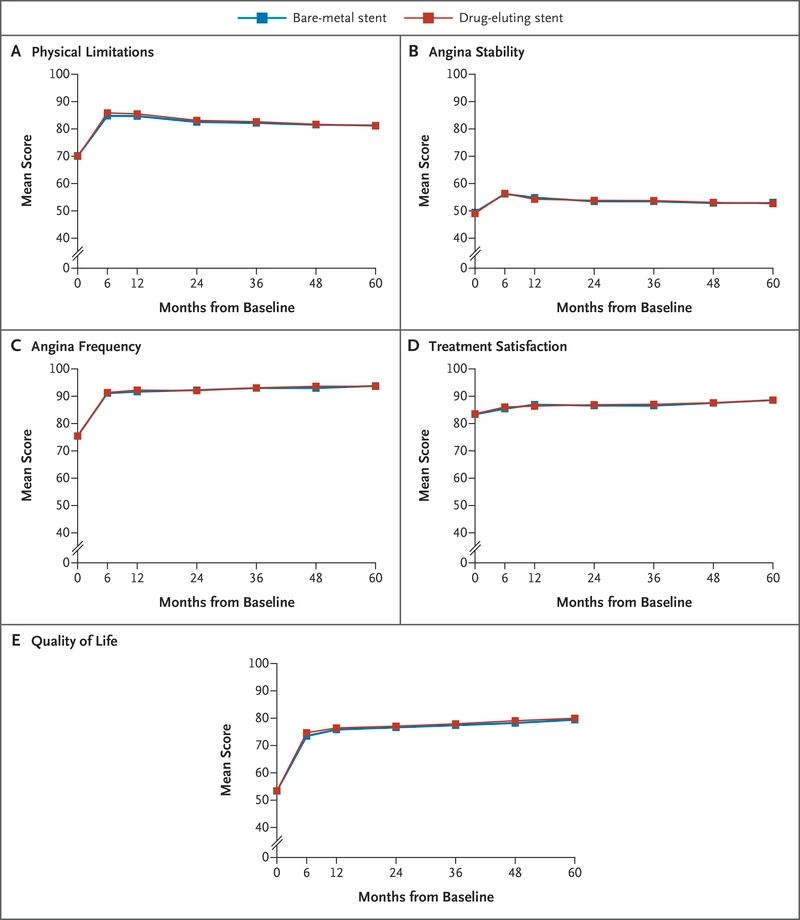 Figure 3. Mean Scores for Disease-Specific Health Status.
Figure 3. Mean Scores for Disease-Specific Health Status.Disease-specific health status was assessed with the use of the Seattle Angina Questionnaire, a 19-item survey that measures five domains of health status related to coronary artery disease: physical limitations, angina stability, angina frequency, treatment satisfaction, and quality of life.20,21 Scores range from 0 to 100, with higher scores indicating fewer symptoms and better health status. There were no significant differences in disease-specific health status between patients assigned to receive drug-eluting stents and those assigned to receive bare-metal stents.
At 6 years, the rates of definite stent thrombosis were low in both groups — 0.8% in the group receiving drug-eluting stents and 1.2% in the group receiving bare-metal stents (P=0.0498); the rates for BARC 3, 4, or 5 bleeding were 5.5% and 5.6%, respectively. Measures of disease-specific health status and quality of life did not differ significantly between the two groups during follow-up (Figure 3, and Table S2 in the Supplementary Appendix).
Discussion
In NORSTENT, we did not find a significant difference between contemporary drug-eluting stents and bare-metal stents in the rates of death from any cause or nonfatal spontaneous myocardial infarction during 6 years of follow-up. The rate of repeat revascularization was significantly lower in the group receiving drug-eluting stents, which showed the durability of this effect over 6 years. Rates of definitive stent thrombosis were low in both groups and appeared to be lower in the group receiving drug-eluting stents than in the group receiving bare-metal stents (P=0.0498). The type of stent had no significant effect on quality of life, as assessed by means of the Seattle Angina Questionnaire. We compared the effectiveness of contemporary drug-eluting stents versus bare-metal stents in a broad group of patients that included more than 72% of those who were eligible, and the study was conducted in the setting of real-world patient care, which supports the generalizability of the results.
In the Basel Stent Kosten Effektivitäts–Prospective Validation Examination (BASKET-PROVE) trial13 involving 2314 patients undergoing PCI, the investigators did not detect a difference between contemporary drug-eluting stents and bare-metal stents in rates of death or myocardial infarction at 2 years of follow-up, although they found a lower rate of target-vessel revascularization in the group receiving drug-eluting stents. Inclusion in that study was restricted to patients requiring larger coronary stents. In the Everolimus-Eluting Stent versus Bare-Metal Stent in ST-Segment Elevation Myocardial Infarction (EXAMINATION) trial7 involving 1504 patients, second-generation everolimus-eluting stents did not reduce the primary end point of death from any cause, recurrent myocardial infarction, or revascularization at 1 year, but rates of stent thrombosis and target-lesion revascularization were significantly lower in the group receiving drug-eluting stents. At 5 years,8 the primary end point was significantly lower in patients receiving drug-eluting stents than in those receiving bare-metal stents, a benefit that was driven mainly by a lower rate of noncardiac death, and there was a nonsignificantly lower occurrence of stent thrombosis.
A higher risk of stent thrombosis has been seen in patients receiving first-generation drug-eluting stents than in those receiving bare-metal stents,4 and the long-term safety of drug-eluting stents has been a concern. NORSTENT contributes to the growing evidence that contemporary drug-eluting stents, as compared with first-generation drug-eluting stents,4 may have a lower risk of stent thrombosis than bare-metal stents,5-10 and demonstrates that this effect persists during long-term follow-up. However, the findings of fewer repeat revascularizations and a potentially lower rate of stent thrombosis with drug-eluting stents did not translate into any difference in the primary outcome or in quality of life, findings that may be explained by the low rates of restenosis and stent thrombosis in the two study groups.
Our trial has several limitations. NORSTENT was an open-label trial, although all outcomes were evaluated by an event committee whose members were unaware of study-group assignments. Patients were recruited during the period from 2008 through 2011, but 95% of the patients in the group receiving drug-eluting stents underwent placement of everolimus-eluting or zotarolimus-eluting stents, which are still commonly used. The quality-of-life data should be interpreted with caution, since the Seattle Angina Questionnaire may not be sensitive enough for evaluation of stent performance. The primary outcome did not include periprocedural myocardial infarction. However, as has been shown in other studies,2 we found that periprocedural myocardial infarction had less prognostic significance than spontaneous myocardial infarction.
In conclusion, in our evaluation of clinical outcomes in 9013 patients with stable or unstable coronary artery disease, we found no significant difference in the 6-year rates of death or spontaneous myocardial infarction between patients receiving contemporary drug-eluting stents and those receiving bare-metal stents. There was also no significant between-group difference in quality of life. The rate of repeat revascularization was lower with the use of drug-eluting stents.
Supplementary Material
| Protocol | 3572KB | |
| Supplementary Appendix | 532KB | |
| Disclosure Forms | 356KB |
References (21)
Citing Articles (242)
Letters
Figures/Media
- Figure 1. Enrollment, Randomization, and Follow-up.
Figure 1. Enrollment, Randomization, and Follow-up. All the patients who were treated with percutaneous coronary intervention (PCI) at Norwegian hospitals from September 15, 2008, through February 14, 2011, were considered for enrollment in the Norwegian Coronary Stent Trial (NORSTENT). Of the 12,425 patients with protocol eligibility, 9013 (72.5%) underwent randomization, with 4504 assigned to receive drug-eluting stents and 4509 assigned to receive bare-metal stents. All the patients were included in the intention-to-treat analyses of the clinical outcomes, and a total of 8969 patients were included in the analyses of disease-specific quality of life.
- Table 1. Characteristics of the Patients at Baseline.
Table 1. Characteristics of the Patients at Baseline. - Table 2. Clinical Events during Follow-up and Cumulative Rates at 6 Years.
Table 2. Clinical Events during Follow-up and Cumulative Rates at 6 Years. - Figure 2. Clinical Outcomes.
Figure 2. Clinical Outcomes. Shown are Kaplan–Meier curves for patients receiving drug-eluting stents and those receiving bare-metal stents for the primary composite outcome of death from any cause and nonfatal spontaneous myocardial infarction (Panel A), death from any cause (Panel B), any revascularization with percutaneous coronary revascularization (PCI) or coronary-artery bypass grafting (CABG) (Panel C), and definite stent thrombosis, as assessed according to the criteria of the Academic Research Consortium (Panel D). The insets show the same data on an expanded y axis.
- Figure 3. Mean Scores for Disease-Specific Health Status.
Figure 3. Mean Scores for Disease-Specific Health Status. Disease-specific health status was assessed with the use of the Seattle Angina Questionnaire, a 19-item survey that measures five domains of health status related to coronary artery disease: physical limitations, angina stability, angina frequency, treatment satisfaction, and quality of life.20,21 Scores range from 0 to 100, with higher scores indicating fewer symptoms and better health status. There were no significant differences in disease-specific health status between patients assigned to receive drug-eluting stents and those assigned to receive bare-metal stents.